10
years after the seminal publication of the Women’s Health Initiative trials data1,
certain facts and data have emerged that can help guide us in this so
controversial an issue of Menopausal Hormonal Therapy (MHT). The following is a
summary of a review published lately in the journal Menopause2.
It
has always been a truth that MHT is an acceptable option for treating severe
early menopausal symptoms. As is the wont of these symptoms, they disappear
within 10 years of menopause, thus this treatment is prudent and applicable within
this time frame. Such therapy must of course be precluded in the presence of
medical problems, foremost of which are blood clots, heart disease, stroke and
cancer.
Estrogen
replacement alone suffices for a woman who has lost her uterus, whereas
progesterone therapy needs to be added for the sole purpose of prevention of
endometrial cancer in those who retain theirs. If the symptoms are limited to
the vulva, vagina and the bladder, topical estrogen therapy to the affected
parts might be enough to soothe the symptoms.
So
much is so true, and we must keep in mind that the whole controversy arose not
because of questionable beneficial effects, rather, the serious consequences of
MHT. Foremost in the mind of most women is the occurrence of breast cancer. The
WHI trials demonstrated an increased risk of breast cancer with more than 5
years continued use of the estrogen-progesterone combination therapy. This
increased risk was not present in users of estrogen-only preparations, thus
suggesting a causal link of breast cancer with progesterone. The data shows
that the risk is not that great and decreases after discontinuation of said replacement
therapy. Estrogen, whether given alone or together with progesterone, increases
the risk of thromboembolic events (TE) such as deep vein thrombosis, pulmonary
embolism and stroke, but these occurrences are rare before the age of 59 years.
Thus
we have come to accept that combination estrogen-progesterone MHT is proven
effective in the management of early menopausal symptoms only (and not for
other indications) but should be used for the shortest duration and with the
lowest possible dosage. More flexibility is accorded to estrogen only therapy
but similar caveats should apply whenever possible.
Fakta Berkenaan Rawatan Hormon Menopause
10 tahun selepas maklumat daripada kajian unggul berkenaan
rawatan menopause diketengahkan1, situasi berkenaan rawatan ini
semakin jelas, saperti dipaparkan dalam jurnal Menopause baru-baru ini2.
Berikut adalah ringkasan tajuk utama.
Terapi hormon untuk menopause (MHT) sungguh berkesan
mengatasi gejala awal menopause dan boleh diteruskan selama 10 tahun, iaitu,
sehingga simptom-simptom keadaan ini hilang. Rawatan ini tidak boleh digunakan jikalau
seseorang wanita mengalami beberapa masalah perubatan, terutama sekali ketulan
dalam saluran darah, serangan angina ahmar, sakit jantung dan kanser.
Rawatan ini boleh dibahagikan kepada 3 – hormon estrogen sahaja
untuk wanita yang tidak mempunyai rahim, kombinasi hormon estrogen-progesteron
bagi mereka yang ada rahim dan krim estrogen setempat jikalau gangguan terhad
kepada kemaluan, faraj atau pundi kencing.
Risiko penggunaan MHT ialah kejadian saperti kanser payudara dan
kejadian tromboembolik (TE) saperti angina ahmar, ketulan darah dan embolasi
paru-paru. Tidak dinafikan yang MHT meningkatkan risiko mengalami kanser
payudara, tetapi jumlah kejadian ini kecil dan risiko tersebut hilang selepas
rawatan diberhentikan. Lagipun, risiko berlakunya kanser payudara hanya meningkat jika digunakan terapi kombinasi estrogen-progesteron dan bukan estrogen
bersendirian. Kejadian TE lebih berkemungkinan berlaku dengan kesemua jenis rawatan
oral tetapi jarang dialami sebelum umur 59 tahun.
Dengan ini, MHT didapati sesuai untuk rawatan simptom-simptom
awal menopause sahaja tetapi perlu digunakan dalam dos yang paling rendah dan
dalam jangkamasa yang paling pendek. Pengawasan untuk gejala kanser payudara dan kejadian TE mesti berterusan.
1. Risks and Benefits of Estrogen Plus Progestin in Healthy
Postmenopausal Women. Principal Results From the Women's Health Initiative
Randomized Controlled Trial. JAMA 2002;288(3):321-333.
2. Stuenkel CA, Gass MLS, Manson J et al. A Decade After the
Women’s Health Initiative – The
Experts Do Agree. Menopause 2012;19(8):846-847.

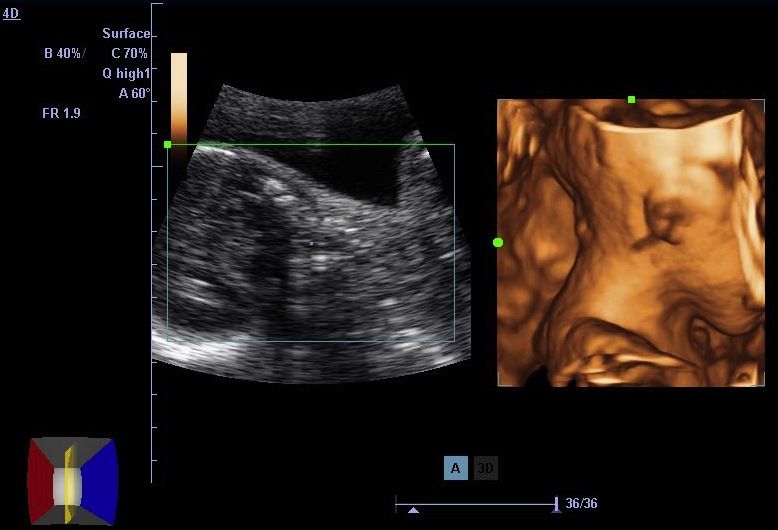
 Ini adalah gambaran yang diambil dari seorang pesakit yang mengadu perasaan sakit dibahagian kiri abdomen. Beliau pernah menjalani pembedahan dan rawatan ubat hormon untuk penyakit endometriosis. Buat masa kini, pesakit ini sedang melalui rawatan kesuburan dengan ubat clomiphene 3 bulan yang lepas yang diberi oleh pakar sakitpuannya. Imbasan ultrasound menampakkan sebuah sista sebesar 9 cm yang mempunyai banyak ruang dalamnya. Ini merupakan sebuah ovari yang telah terangsang berlebihan oleh ubat clomiphene. Rangsangan hiper saperti ini jarang belaku dengan ubat clomiphene dan biasa surut tanpa komplikasi. Tindakan utama ialah pemerhatian dan elak dari melakukan pembedahan tergesa-gesa.
Ini adalah gambaran yang diambil dari seorang pesakit yang mengadu perasaan sakit dibahagian kiri abdomen. Beliau pernah menjalani pembedahan dan rawatan ubat hormon untuk penyakit endometriosis. Buat masa kini, pesakit ini sedang melalui rawatan kesuburan dengan ubat clomiphene 3 bulan yang lepas yang diberi oleh pakar sakitpuannya. Imbasan ultrasound menampakkan sebuah sista sebesar 9 cm yang mempunyai banyak ruang dalamnya. Ini merupakan sebuah ovari yang telah terangsang berlebihan oleh ubat clomiphene. Rangsangan hiper saperti ini jarang belaku dengan ubat clomiphene dan biasa surut tanpa komplikasi. Tindakan utama ialah pemerhatian dan elak dari melakukan pembedahan tergesa-gesa.